










Article
Dermoscopy of Early Stage Melanoma
Melanoma develops from melanocytes, which are located in the epidermis of the skin. Melanoma can be display as changes of existing mole or a new spot on the skin. If not identified and treated early, melanoma is more likely to spread to other parts of the body. Melanoma can become life-threatening even in 6 weeks…
Clinical Guide to Early Stage Melanoma Dermoscopy and Diagnostic Accuracy
In the field of dermatology, early stage melanoma dermoscopy represents the single most effective non-invasive method for reducing mortality rates. Early detection is not merely a clinical goal; it is a diagnostic necessity that requires the identification of subtle morphological changes before they become visible to the naked eye. By utilizing high-resolution optical systems, clinicians can bridge the gap between initial screening and histopathological confirmation.
The challenge of early stage melanoma dermoscopy lies in distinguishing between atypical melanocytic nevi and early-stage malignancies. This guide delves into the hallmark patterns, systematic algorithms, and technical requirements necessary for providing precise patient care and achieving clinical confidence.
Hallmark Patterns in Early Stage Melanoma Dermoscopy
The diagnostic process involves a meticulous search for a combination of atypical features. Unlike mature lesions, early-stage malignancies often present with discrete clues that require high-grade magnification and polarized lighting to resolve.
1. The Evolution of Atypical Pigment Networks
The pigment network is the primary focus during an initial examination. In benign lesions, the network is typically delicate, symmetrical, and fades gradually at the periphery. However, in early stage melanoma dermoscopy, clinicians must look for:
- Irregular Spacing and Thickness: The network lines appear uneven, with focal areas of thickening and increased pigmentation density.
- Abrupt Peripheral Termination: A critical red flag where the network stops suddenly at the lesion's edge rather than fading out, often indicating an invasive growth pattern.
- Multicomponent Patterns: The presence of different structural zones within a single lesion, reflecting the clonal heterogeneity of malignant cells.
2. Vascular Morphology and Neoangiogenesis
As a tumor begins to develop its own blood supply, atypical vascular patterns become visible. Early stage melanoma dermoscopy frequently reveals "dotted" or "linear-irregular" vessels. These vessels are often chaotically distributed and vary in caliber, a clear departure from the organized vascularity seen in inflammatory conditions or benign nevi.
3. Regression Structures and the Blue-White Veil
Regression is a biological hallmark of melanoma evolution. Under the dermoscope, this manifests as "peppering" (blue-gray granules) or the blue-white veil. The blue-white veil is a hazy, structureless area that reflects either deep dermal pigment or orthokeratosis over a highly cellular tumor, making it one of the most specific indicators for malignancy.
Systematic Evaluation: The 7-Point Checklist and ABCD Rule
To standardize early stage melanoma dermoscopy, several validated algorithms are utilized. The 7-point checklist is particularly effective for high-risk screening, focusing on major criteria such as atypical network, blue-white veil, and atypical vascular patterns.
The ABCD rule—scoring Asymmetry, Border irregularity, Color variation, and Dermoscopic structures—provides a quantifiable framework for deciding when a biopsy is necessary. In the context of early stage melanoma dermoscopy, a total score exceeding 4.75 typically prompts an immediate surgical excision to rule out in-situ or thin invasive melanoma.
Site-Specific Challenges: Facial and Acral Locations
The clinical appearance of early melanoma is heavily influenced by its anatomical location. On facial skin, the absence of a classic pigment network requires clinicians to focus on annular-granular patterns and asymmetric follicular openings. Conversely, in acral locations (palms and soles), early stage melanoma dermoscopy is defined by the parallel ridge pattern—where pigment occupies the ridges of the skin markings rather than the furrows—a finding with high diagnostic specificity.
Technology and Precision: Why Optics Matter
The accuracy of early stage melanoma dermoscopy is fundamentally tied to the quality of the instrument. High-grade optics, such as those found in IBOOLO professional dermatoscopes, ensure that subtle regression structures and fine vascular patterns are not lost to chromatic aberration or poor illumination.
IBOOLO Advanced Imaging: Our devices, including the DE-4100 series, provide the cross-polarization required to eliminate surface glare without the need for immersion fluids. This mobility, combined with smartphone integration, allows for Sequential Digital Dermoscopy Imaging (SDDI). By comparing 4K images over a 3-to-6-month interval, clinicians can detect the "evolving" (E) criterion of melanoma at its most treatable stage.
Diagnostic Accuracy and Evidence-Based Outcomes
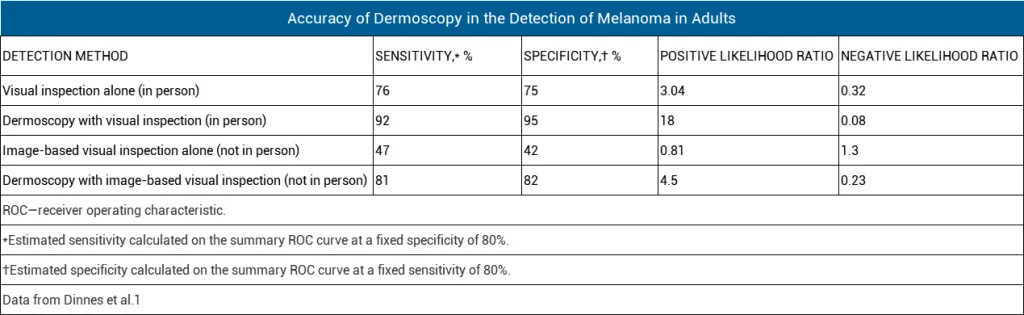
Clinical research, including the 2018 Cochrane meta-analysis, confirms that the use of dermoscopy improves the sensitivity of melanoma detection to 92%, compared to 76% for naked-eye examinations alone. For early stage melanoma dermoscopy, this 16% gap represents a significant number of lives saved through early intervention and the reduction of unnecessary biopsies for benign lesions.
Early stage melanoma dermoscopy is a sophisticated process of pattern recognition that requires both high-quality diagnostic tools and clinical expertise. At IBOOLO, we are dedicated to providing the optical precision needed to empower clinicians in the early detection of skin cancer.
Recommended reading
dermoscopy melanoma – IBOOLO
Shenzhen Iboolo Optics Co.Ltd established in 2012, with more than 11+ years. We have been specialized in the field of Dermatoscope, Microscope, Macro lens and Woods Lamp, and so on. We are a high-tech company integrated with research, manufacture and marketing.
Shipping Estimates – IBOOLO
For in-stock items, Expected Delivery Dates are provided for each shipping option during checkout. Expected delivery dates are estimates. Orders may be delayed due to verification protocols, weather, customs delays, or the time of order placement. Stock exceptions cannot be held to expected delivery dates. Orders may be delivered in separate shipments. These...
Top Download DE-3100 User Manual supplier & manufacturer – IBOOLO
IBOOLO is a Top Download DE-3100 User Manual supplier & manufacturer. Information for Download DE-3100 User Manual: DE-3100 user manualDownload...
Melanoma develops from melanocytes, which are located in the epidermis of the skin. Melanoma can be display as changes of existing mole or a new spot on the skin. If not identified and treated early, melanoma is more likely to spread to other parts of the body. Melanoma can become life-threatening even in 6 weeks due to its aggressive speed of growth.
Hence, there is very crucial to inspect melanoma in its early stage. Dermoscopy is a very reliable and valuable aiding tool to identify and diagnose early melanoma. Dermoscopy enhances the confidence of dermatologists and patients, and also reduces the unnecessary biopsy and surgery.
What is melanoma?
Melanoma is a type of potential dangerous skin cancer that originates from melanocytes. Melanocytes are cells that are responsible for producing pigment melanin and give color to the skin. When melanocytes start to grow out of control, then melanoma arises. As a potential invasive skin cancer, melanoma can spread very quickly to other tissues of the body if left untreated.

What is early melanoma?
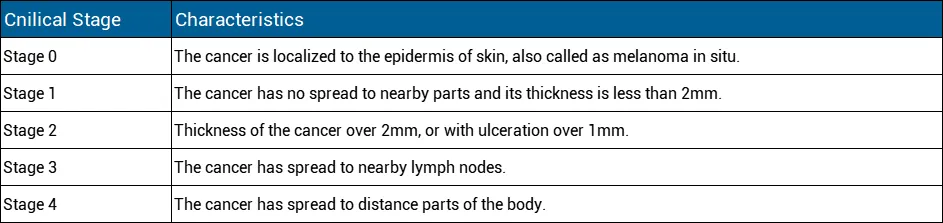
Early melanoma means it is on the early stage, has not spread. Stage of 0 and 1 are the early stage of melanoma
Stage 0: Stage 0 is the most noninvasive stage of melanoma, also called melanoma in situ. Such melanoma is located in the outermost layer of the skin and has not developed deeper.
Stage 1: Early melanoma, although also localized, becomes aggressive when it has penetrated the surface layer into the next layer of skin. At this point, the invasive tumor is less than 1 mm in size and may or may not ulcerate. When it is not ulcerated and is less than 0.8 mm in size, it is considered early and thin, also known as stage 1.
Epidemiology of melanoma
In the world, incidence rates of melanoma has been rising, especially like Australia and New Zealand reported as the highest rate of c
ountries. Western European and North America are following. Meanwhile, Asia and Africa have lower incidence rate of melanoma. As reported, melanoma is the third most common cancer in Australia and New Zealand. Melanoma is the fifth most common cancer in America.
Fair-skinned populations are the higher risk of groups than dark-skinned people in general.
High risk of melanoma
The main high risk factor for developing melanoma is over UV exposure, otherwise, there are some other high risk factors for producing melanoma as below:
Over UV exposure/history of sunburn
Fair-Skinned /white-skinned population
Family history
Existing moles
Increasing age
Weakened immune system
Clinical signs of early melanoma
The first clinical signs and symptoms of melanoma commonly are:
A change in an existing mole or freckle
The appearance of a new spot or atypical looking growth on the skin
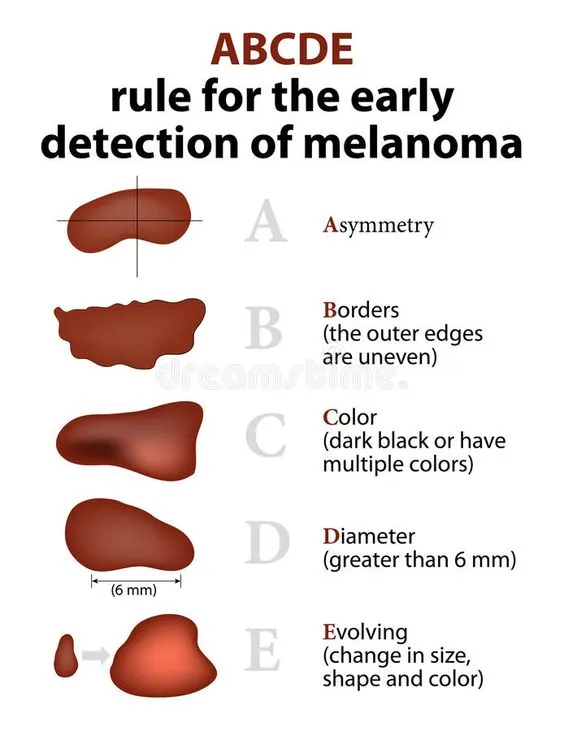
For early melanoma, there are famous “ABCDE” rules of the signs include: A: A is for Asymmetry. Melanoma often has irregular shapes and its two half are asymmetric. It means one half can not match the other. B: B is for Border. Border are irregular, blurred or ragged.
C: C is for Color. Colour is fulled with variation, or unusual colors, mixed colors and may change over the time.
D: D is for Diameter. Diameter of the spot is larger than 1/4inch (about 6millimeters)
E: E is for Evolving. Melanoma is change in its size, shape or color over time.
Stages of early melanoma
Stages of early melanoma can be complex, in summary, the stages are:
Dermoscopy of early stage melanoma
In clinical, some melanomas are extremely complex and difficult to identify. Especially in early stage of melanoma, its appearance in small size hard to detected. Dermoscopy plays a very important role to identify and diagnose the melanoma by combining a powerful lighting system and great magnification.
There are some certain features of early melanoma under dermoscopy including:
Asymmetrically distributed
Unusual pigment network
Irregular brown-black or multiple dots/globules
Blue-white veil
atypical vascular pattern or radial streaming
Scar-like depigmentation

What is the technique of dermoscopy?
Dermoscopy, also known as dermatoscopy or epiluminescence microscopy, is a dependable and useful medical device of helping skin doctors to diagnose various of skin lesions or skin diseases. Here’s the technique of dermoscopy as below:
Instrument: Dermoscopy is commonly display as a handheld tool. This tool combines magnifying lens with a powerful lighting system to allow enhanced visualization with more details that are invisible by naked eyes. In addition, some dermoscopes is designed attached on a camera or a phone to directly observe or capture images of skin lesions.
Skin Preparation: Before the examination of dermoscopy, the patient’s skin should be keep clean. In some cases, if necessary, hair should be removed.
Application of Gel or Fluid: A gel or liquid (often alcohol or oil) may be applied to the skin lesion to reduce surface reflections and allows better visualization of deeper skin. But with the innovation and development of dermoscopy, there might no need any gel or liquid during the process of dermoscopy examination.

Observation of Structures: Dermoscopy reveals details of specific structures of the lesion to supply more valuable and key information for diagnosis.Such details include pigment networks, dots, globules, vessels, and other patterns.
Digital Imaging: Some dermoscopes are connected with a computer or a phone to capture digital images of the skin lesion. These images can be stored for later analysis and comparison.
Training and Expertise: It requires specialized and trained medical workers to interpret dermoscopic findings. Various patterns of dermatoscopic features of the lesion should be correlated with clinical context to get accurate and precise diagnosis.
How accurate is dermoscopy for melanoma?
Inspection by dermoscopy is more accurate than visual inspection alone in the diagnosis of melanoma.The accuracy of dermoscopy has been reported to range from 60% to 100%. But generally, Dermoscopy improved the accuracy of clinical diagnosis up to 35%.
A 2018 Cochrane meta-analysis evaluated the diagnostic accuracy of dermoscopy in melanoma.
Advantages and disadvantages of dermoscopy for melanoma
As we can see, dermoscopy indeed can increase the sensitivity of diagnosis for melanoma.There are some advantages and disadvantages of for comparison dermoscopy with clinical examination(visual inspection):
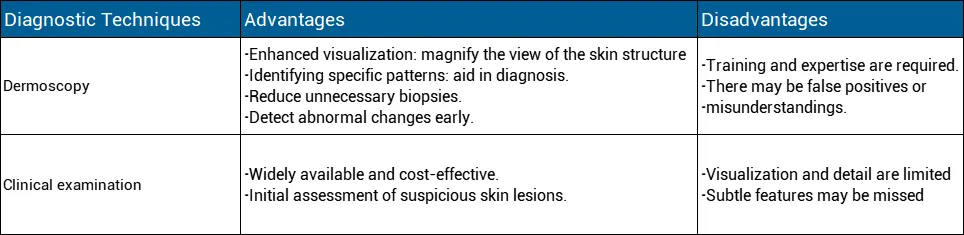
Compared with clinical examination, dermoscopy allows a brightening detail structures of skin lesion which are invisible by naked eyes. It is no doubt that dermoscopy can greatly increase the accuracy of diagnosis. In addition, dermatologist can store the images captured by dermoscope connected with phone or computer for later analysis and comparison. Dermoscopy plays a very significant role in the detection and diagnosis of skin lesion. People also need to learn how to use a dermoscopy to do self-examination in daily life . Any suspicious findings, have the skin checked by the professionals as soon as possible.











