Case for iPhone – IBOOLO
People May Ask
The hair growth process is irreversibly halted due to the comprehensive deterioration of the hair bulb by scar tissue. The underlying mechanism involves the annihilation of vital structures such as stem cells and sebaceous glands, situated atop the hair bulbs, during inflammatory episodes surrounding the hair follicles. Consequently, hair follicles are rendered incapable of further growth, resulting in permanent hair loss.
In conclusion, the investigation revealed the superiority of Itracanazole's efficacy over terbinafine, albeit both medications are viable options for treating Tinea corporis. Consequently, this study advocates for the employment of Itracanazole in addressing Tinea-related conditions. Notably, both treatment groups exhibited no significant adverse effects.
As an illustration, there can be instances where tinea corporis may be erroneously mistaken for eczema, whereas tinea capitis may be confused with alopecia areata, and furthermore, onychomycosis could be misconstrued as dystrophic toenails stemming from recurrent minor injuries. Hence, it is imperative for medical practitioners to ascertain cases of suspected onychomycosis and tinea capitis through the utilization of potassium hydroxide preparations or cultural tests.
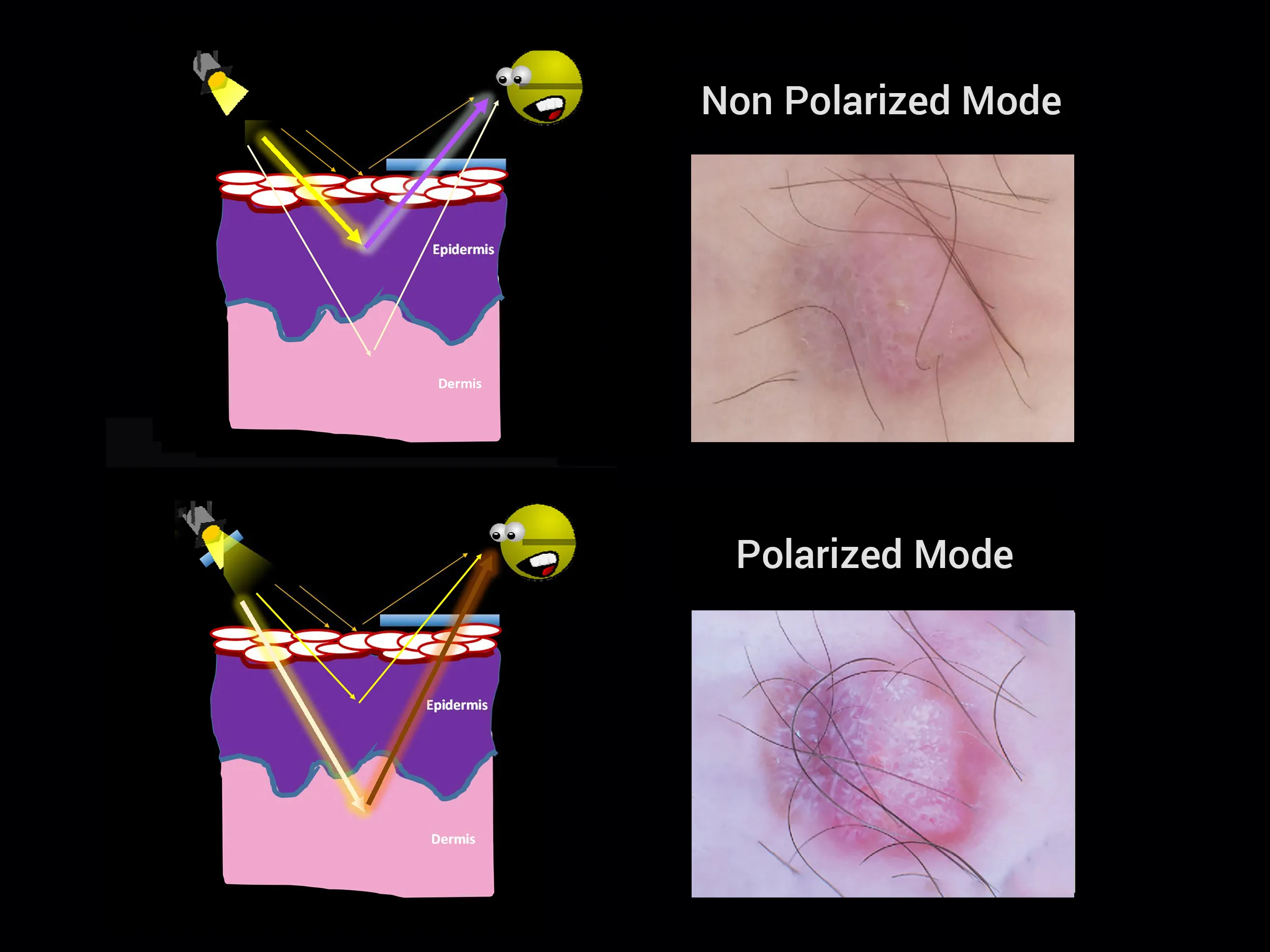
Summarizing the Significance and Relevance, diagnosing melanomas that mimic seborrheic keratosis (SK) through dermoscopy can pose intricate challenges. However, the identification of key indicators such as the blue-black hue, intricate pigment network patterns, pseudopodial or streak-like formations, and/or the presence of a blue-white veil, even amidst other typical SK characteristics, facilitates accurate diagnosis in the majority of intricate melanoma instances.
A Comprehensive Overview of Medication Utilization
Historically, griseofulvin has stood as the premier therapeutic approach for addressing all instances of scalp ringworm infections. A comprehensive analysis conducted in 2008 reaffirms its efficacy, establishing griseofulvin as a dependable treatment option for tinea capitis. Dated October 2, 2024.
The distinctive differential evaluation for tinea corporis encompasses: Discoid dermatitis, Psoriasis vulgaris, and the herald patch observed in Pityriasis rosea.
Histopathologically, the structure of single-cell squamous cell carcinoma (SCC) is predominantly comprised of individual, atypical cells that either reside solitarily or form loosely packed clusters within the dermal layer. A conspicuous absence of cohesion among these atypical cells is evident, typically devoid of any linkage to the superjacent epidermis or adjacent appendageal structures.
What comprises the comprehensive differential diagnosis for tinea capitis? This diverse list encompasses a broad range of conditions that could potentially manifest with symptoms such as patchy hair loss, inflammation, and scaling of the scalp. Illustrative instances encompass Alopecia areata and trichotillomania, both of which lead to patchy alopecia but do not involve scaling.
The origins of Tinea capitis trace back to the emergence of a minute erythematous papule, situated proximally to a hair follicle, on the scalp, eyebrows, or eyelashes. Over the course of several days, this initial red lesion undergoes a transformation, acquiring a paler hue and becoming covered in scales. Subsequently, the hairs exhibit discoloration, lose their shine, and develop a fragile quality, ultimately breaking off at a distance of mere millimeters above the scalp's surface.
Griseofulvin stands as the primary oral therapeutic agent employed in the management of tinea capitis, particularly targeting Trichophyton strains. Widely acknowledged as the "gold benchmark," this medication has held the foremost position in physicians' prescriptions for over half a century(4), serving as the cornerstone of treatment for affected individuals.