










Article
What are the Common Skin Cancers?
Skin cancer stands out as the most prevalent form of cancer globally, with millions of new diagnoses annually. Unlike many other cancers, skin cancer often presents visible signs, making early detection feasible. The American Cancer Society reports a steady rise in skin cancer incidence over recent decades. Among these, basal cell carcinoma (BCC), squamous cell…
Skin cancer stands out as the most prevalent form of cancer globally, with millions of new diagnoses annually. Unlike many other cancers, skin cancer often presents visible signs, making early detection feasible. The American Cancer Society reports a steady rise in skin cancer incidence over recent decades. Among these, basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma are the most frequently encountered types. BCC is the most common, accounting for approximately 80% of all skin cancers. SCC follows, making up around 20%, while melanoma, though less common, is the most aggressive and deadly. Early detection and treatment are vital for favorable outcomes and reduced complications.
What is Basal Cell Carcinoma?
Basal cell carcinoma (BCC) originates from the basal cells of the interfollicular epidermis and/or hair follicle. It is the most common type of skin cancer, accounting for about 80% of all skin malignancies. BCC can arise anywhere on the body but is most commonly seen on sun-exposed areas such as the face, neck, and arms. It typically presents as a slow-growing, pearly or flesh-colored nodule or plaque, which may ulcerate and bleed. BCC rarely metastasizes but can cause significant local tissue destruction and disfigurement if left untreated.
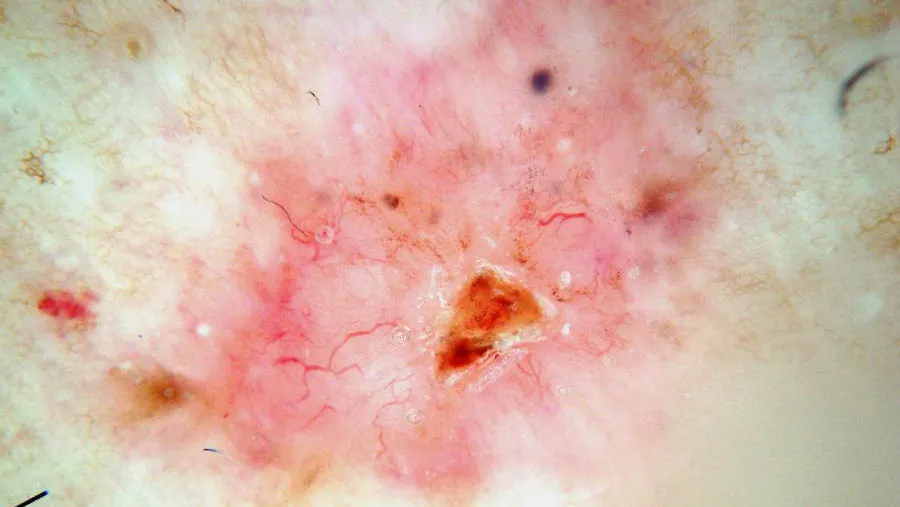
What are the Dermatoscopic Features of Basal Cell Carcinoma?
The dermoscopic features of BCC vary according to subtype. Pigmented BCC may exhibit features such as absence of pigment network, linear and arborizing telangiectasia, structureless or leaf-like areas on the periphery of the lesion, large blue-grey ovoid nests or blotches, multiple blue-grey globules, specks of brown and grey pigment, spoke wheel areas, and focal ulceration. Nonpigmented BCC typically shows bluish or whitish-pink stroma, asymmetrical branching serpentine vessels, focal ulceration, slight scaling, and white clues, particularly perpendicular white lines under polarized light and structureless roundish white or yellowish areas.
What is Squamous Cell Carcinoma?
Squamous cell carcinoma (SCC) is another common type of skin cancer that arises from the keratinocytes of the epidermis. It is the second most common skin cancer, accounting for approximately 20% of all skin malignancies. SCC most often occurs on sun-exposed areas such as the face, ears, neck, hands, and forearms. It typically presents as a red, scaly plaque or nodule, which may ulcerate and have a crusted surface. SCC can metastasize, especially in high-risk populations such as immunocompromised individuals.
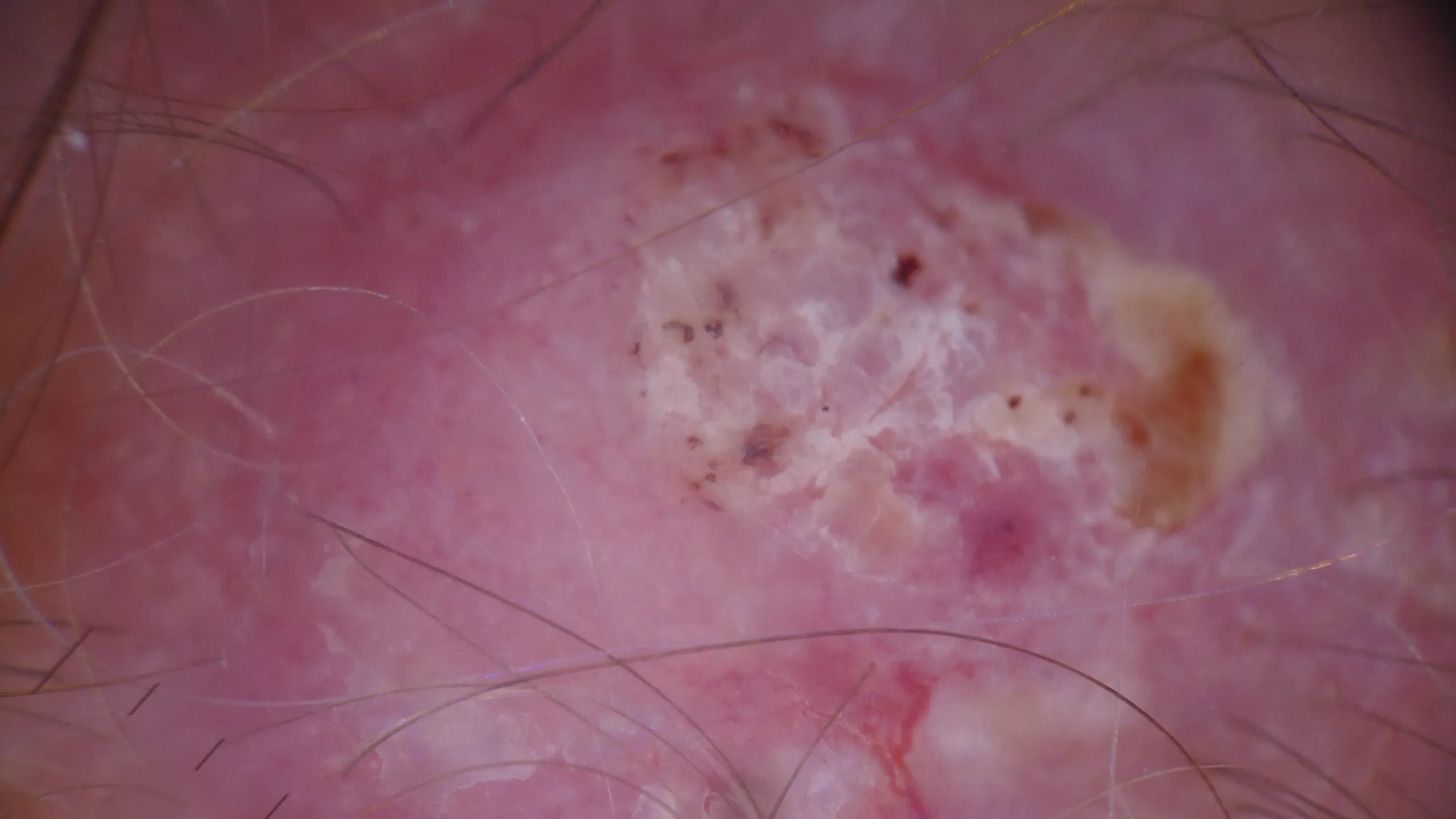
What are the Dermatoscopic Features of Squamous Cell Carcinoma?
The dermoscopic features of SCC may include well-defined borders, hyperkeratosis, scaling, erythema, and the presence of ulceration. Vascular patterns such as glomerular vessels or irregular dotted vessels may also be observed. SCC often shows asymmetry and pleomorphic vessels, which are important clues for diagnosis. Under polarized light dermoscopy, SCC may reveal additional features such as structureless areas, white patches, and keratin globules.
What is Melanoma?
Melanoma is a malignant tumor that arises from melanocytes, the cells responsible for producing melanin. It is less common than BCC and SCC but is the most aggressive and deadly form of skin cancer. Melanoma can occur anywhere on the body, including non-sun-exposed areas. It often presents as an asymmetric, irregularly bordered, multicolored mole or lesion. Early detection and treatment are critical for improving survival rates, as melanoma can metastasize rapidly to other parts of the body.
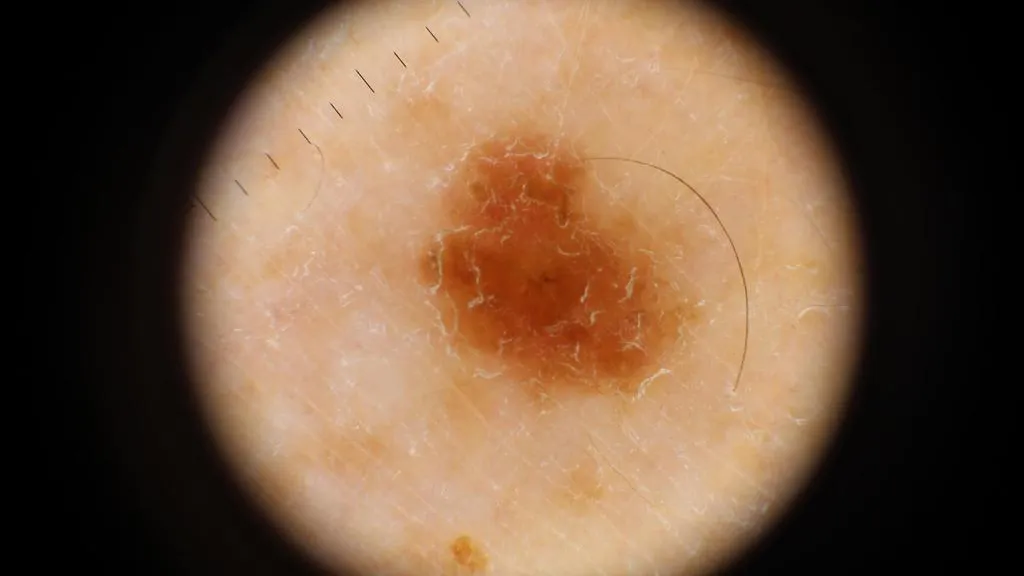
What are the Dermatoscopic Features of Melanoma?
The dermoscopic features of melanoma are diverse and can vary depending on the subtype and stage of the lesion. Common features include asymmetry, irregular borders, multiple colors (brown, black, blue, red, white), and specific structures such as atypical pigment networks, blue-black areas, and white or pink structureless areas. The presence of regression structures (e.g., blue-gray globules, black dots, and patches) and asymmetric follicular openings are also important indicators. In nodular melanoma, features such as a homogeneous blue-black or black color, irregular blotches, and multiple blue-black globules are often observed. For lentigo maligna melanoma, the presence of a broad and irregular pigment network, gray lines, pseudopodia, and multiple blue-gray globules at the periphery is characteristic. Acral lentiginous melanoma typically shows parallel ridge dermoscopic patterns, intersecting white lines, and multiple blue-black dots or globules.
Is Dermatoscopy Effective for Skin Cancer?
Dermatoscopy is a non-invasive diagnostic technique that has revolutionized the detection and management of skin cancer. IBOOLO handheld dermatoscopes are capable of 10X magnification. They can reveal subtle details that are invisible to the naked eye. The IBOOLO DE-4100 has a variety of light modes, polarized light, unpolarized light, amber light, which can basically satisfy the observation of all skin lesions.
The ability to observe specific features like asymmetric borders, irregular pigmentation, and unusual vascular patterns helps in distinguishing benign lesions from malignant ones. Dermatoscopy not only improves diagnostic accuracy but also reduces the need for unnecessary biopsies by providing clearer information about the nature of a skin lesion.











