










Article
Dermoscopy of Pigmented Basal Cell Carcinoma
Pigmented basal cell carcinoma refers to a subtype of basal cell carcinoma characterized by the presence of significant amounts of melanin within the tumor and in the surrounding stromal melanophages. It is an uncommon variant of BCC, with a lower incidence rate and usually presents as pigmentation at the site of lesion. PBCC may present…
Clinical Guide: Mastering the Dermoscopy of Pigmented Basal Cell Carcinoma (BCC)
In contemporary dermatological diagnostics, the dermoscopy of bcc has become the gold standard for early detection, particularly for the pigmented variant. Pigmented basal cell carcinoma (PBCC) accounts for a significant percentage of BCC cases in populations with higher skin phototypes, often presenting a diagnostic challenge due to its ability to mimic melanoma, blue nevi, and seborrheic keratosis.
At IBOOLO, we recognize that accurate pigmented bcc dermoscopy requires high-resolution imaging to resolve subtle morphological structures. This guide explores the diagnostic criteria, vascular archetypes, and clinical patterns necessary for precise non-invasive diagnosis.
Key Morphological Features in Pigmented BCC Dermoscopy
The diagnostic accuracy for PBCC via dermoscopy is significantly higher than visual inspection alone. According to the Menzies criteria, the diagnosis of pigmented bcc dermoscopy is based on the absence of a pigment network and the presence of at least one of the following classic features.
1. Arborizing Telangiectasias
Commonly referred to as the most specific vascular sign of BCC, these are bright red, sharply focused, and branching vessels that resemble the limbs of a tree. In cases of pigmented bcc dermoscopy, these vessels are typically found at the periphery or on the surface of the lesion, best visualized through cross-polarized lighting.
2. Large Blue-Gray Ovoid Nests
These are well-demarcated, rounded or oval-shaped areas of pigmentation that lack a connection to any pigment network. They appear as dark brown or bluish-gray masses and represent large aggregations of basaloid cells within the dermis.
3. Maple Leaf-like and Spoke-Wheel Areas
Maple leaf-like areas are discrete, brown-to-grayish bulbous structures often located at the lesion's edge. Similarly, spoke-wheel areas consist of well-circumscribed pigment structures radiating from a dark central point. These features are highly specific to pigmented bcc dermoscopy and are seldom seen in other malignant or benign lesions.
Differential Diagnosis: Pigmented BCC vs. Mimickers
The power of dermoscopy of bcc lies in its ability to differentiate suspicious lesions. The table below summarizes the critical findings that distinguish PBCC from melanoma and benign nevi.
| Feature | Pigmented BCC | Malignant Melanoma |
|---|---|---|
| Vascularity | Arborizing / Branching | Polymorphous / Dotted |
| Pigment Network | Absent | Present (Atypical) |
| Specific Signs | Ovoid Nests / Spoke-Wheel | Regression / Pseudopods |
| Symmetry | Often Asymmetric | Highly Asymmetric |
Clinical Case Analysis and Histological Correlation
Effective dermoscopy of bcc often reflects histopathological changes. For example, blue-gray globules and spherules correspond to smaller dermal nests of tumor cells containing melanin. Utilizing a high-resolution dermatoscope with 4K imaging capability, such as the IBOOLO DE-4100 Pro, ensures that these minute structures are not missed during a routine screening.
Clinicians should adopt a systematic workflow when performing pigmented bcc dermoscopy:
- Initial Polarization: Use polarized light to visualize the deeper arborizing telangiectasias.
- Pattern Identification: Scan the margins for maple leaf-like or spoke-wheel structures.
- Longitudinal Comparison: Store high-definition images for sequential monitoring of evolving lesions.
Mastery of the dermoscopy of bcc and the nuances of pigmented bcc dermoscopy allows clinicians to provide life-saving care while reducing the rate of unnecessary biopsies. At IBOOLO, we are committed to providing the optical precision required for high-stakes diagnostic environments.
Recommended reading
Smartphone DE-200 dermatoscope for mobile skin Imaging - IBOOLO
IBOOLO The DE-200 smartphone dermatoscope easily attaches to your mobile phone, transforming it into a handheld tool for high-quality dermoscopy and skin analysis.
Dermoscopy Applications in the Diagnosis of Psoriasis - IBOOLO
IBOOLO Discover the powerful role of dermoscopy in diagnosing and managing psoriasis. Explore the distinctive dermoscopic features that aid in early detection and differentiation from similar skin conditions.
Dermoscopy of Seborrheic Keratosis – IBOOLO
Seborrheic keratosis is a common skin hyperplasia. It is often mistaken for a disease such as skin cancer because of its appearance that looks like warts, precancerous skin growths, or skin cancer. Dermoscopy of seborrheic keratosis is crucial to identify seborrhei keratosis from other types of skin diseases. What is Seborrheic Keratosis?Seborrheic keratosis...
Pigmented basal cell carcinoma refers to a subtype of basal cell carcinoma characterized by the presence of significant amounts of melanin within the tumor and in the surrounding stromal melanophages. It is an uncommon variant of BCC, with a lower incidence rate and usually presents as pigmentation at the site of lesion. PBCC may present initially as only mild pigmentour alterations and slight skin changes, which could possibly remain unrecognizable. Because dermoscopy is extremely sensitive, it can find these subtle changes and thus allows to detect this earlier.
What is pigmented basal cell carcinoma?
Epidemiologically, pigmented basal cell carcinoma occurs more frequently with increasing age. In addition, risk factors involved in the PBCC pathogenesis include chronic malady of sun exposer (sunbathing), presence of ultraviolet radiation and ionizing Radiation, Chemical contamination; outside stimuli are included with genetic factor. PBCC is the most challenging because early diagnosis and treatment are critical. Although the disease had a low-grade malignant potential, untreated PBCC could cause much harm to its carrier.
The most distinct difference between pigmented basal cell carcinoma and other forms of basal cellular carcinomas (such as nodular ulcerative type, superficial type) is the prominent hyperpigmentation of the lesions in contrast to those that show mostly different colors rather than black. Compared with non-pigmented basal cell carcinoma, the incidence of pigmented BCC is low.

Advantages of dermoscopy in the diagnosis of pigmented skin lesions
The basic principle of dermoscopy is the use of optical magnification to avoid reflected light from then surface and provide enlargement on fine structures at the skin surface, allowing a deeper look further beyond stratum corneum or even in superficial dermis. Dermoscopy should be done under the supervision of a dermatologist. The skin in the lesion area should be relatively dry before examination, and lubricants or ointments are not applied.
This technique visualizes skin structures that are not easily observed by the naked eye, including a detailed dermatoscopic view of pigment networks and vascular patterns among other important diagnostic landmarks to aid in early diagnosis from melanomas and pigmented basal cell carcinoma. Moreover, dermoscopy is a non-destructive and elegant process that involves no pain or harm to the patient. Dermoscopy is a simple, quick and inexpensive method as compared to other screening methods.
Dermoscopic features of pigmented basal cell carcinoma
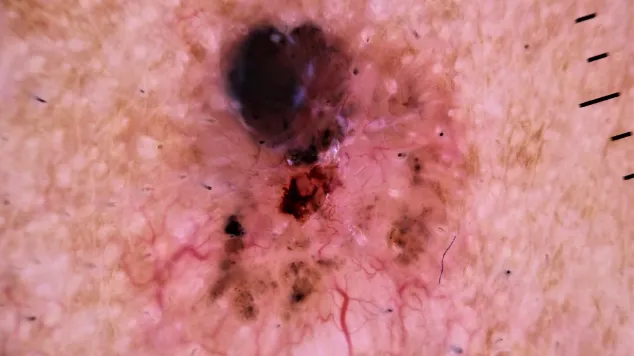
Blue-gray globules: dermoscope might sometimes show large, round or oval structures which appear to be filled with melanin reflected as bluish-grey.
Dendritic blood vessels: a dermoscopic hallmark of basal cell carcinoma, also seen in pigmented BCC. This pattern is dendritic and originates from a central point, making it very distinctive.
Pigmentation network: PBCC often shows a lack of a typical pigmentation network; instead, it may appear as an unstructured or foliated area around the lesion.
Differences between pigmented basal cell carcinoma and other pigmented skin lesions
Dermoscopy allows the visualization of features crucial to distinguishing PBCC from other pigmented lesions
(1). Melanoma.
Appearance: The lesion is asymmetrical with irregular borders and many colors (brown, black, blue, red ).
Dermoscopy: Atypical pigmentation network, irregular streaking with blue-white veil.
Difference: PBCC typically shows blue-gray blobs, dendritic vessels surrounding usual pigment network
(2). Blue nevus.
Appearance: A unique lesion that is blue or black
Dermoscopy: Uniform blue pigmentation without any structure
Distinction: PBCC has additional features such as dendritic vessels and blue-gray ovoid nests
(3). Solar Lentigo.
Appearance:Brown macules that are flat and often found in sun-exposed sites
Dermoscopy: A fine mesh pattern of uniform pigmentation.
Difference: PBCC demonstrates a more complex arrangement of blue-gray globules and dendritic blood vessels
Interpretation difficulties and common pitfalls in dermoscopic images of pigmented basal cell carcinoma
The resultant dermoscopic image of PBCC generally shows a complex structure with various types of blue-grey blobs and dendritic blood vessels, which demand very-rich experience as well as expertise in the identification and interpretation process. Moreover, dermoscopic features of PBCC may resemble some benign lesions like blue nevi and pigmented nevus which should be accurately differentiated in reading.
During interpretation of dermoscopic images, some doctors may focus too much on a single criterion (e.g., blue-gray blobs) and ignore other clinical data or notable features observed through polarisation analysis. Moreover, pigmented basal cell carcinoma also presents as a black papule or nodule and its dermoscopic image resembles that of melanoma. Consequently, sometimes a biopsy is done to differentiate pigmented basal cell carcinoma from melanoma.
A clinical case of pigmented basal cell carcinoma
Case Presentation
Patient: 65-year-old male with a long history of sun exposure and pigmented lesion on left cheek. It has been slowly growing larger for the last 12 months.
Examination: 1.5 cm ill-defined dark plaque with a sclerotic surface
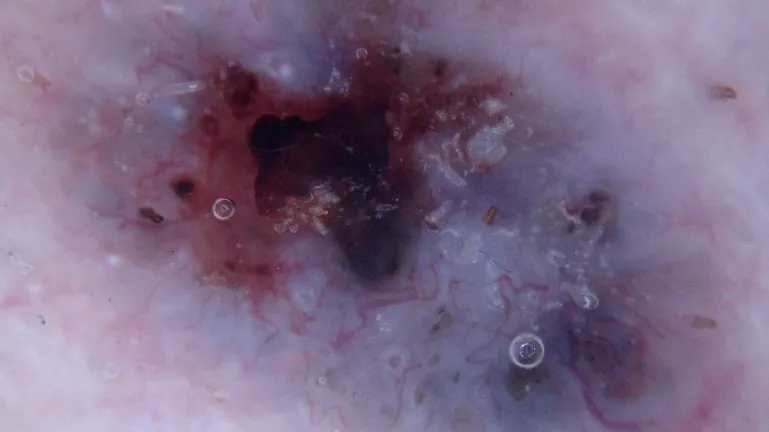
Dermoscopic examination:
(1) A bluish or grayhill to brown net is observed which has a different color and intensity in the various areas of the plaque.
(2) Multiple blue-gray spherules irregularly arranged and surrounded by normal skin
(3) Maple-like appearance at edges of the plaque with tiny dendritic blood vessels distributed in marginal areas.
Diagnostic process:
Preliminary Diagnosis: Clinical and dermatoscopic features were consistent with the diagnosis of pigmented basal cell carcinoma.
Further Examination: A biopsy from the margin of plaque was obtained under local anesthesia.
Histopathological Results: Pathological sections showed the presence of a tumor mass in the dermis composed of basal-like cells. Melanocytes were seen in the tumor parenchyma and melanophagocytes were seen in the interstitium, consistent with pigmented basal cell carcinoma.
Diagnosis:
He was eventually diagnosed with pigmented basal cell carcinoma.
Association between dermoscopic and histologic features
Pigmented lesions: Dermoscopic features of pigmented lesions often reflect the proliferation, distribution and arrangement of melanocytes within the lesion, as well as the morphology and density of blood vessels.
Non-pigmented lesions: The dermoscopic features of non-pigmented lesions are often associated with changes in cellular components such as keratinocytes and fibroblasts within the lesion.
Vascular structure: Dermoscopic features of vascular structure are often consistent with histopathologic changes in vascular morphology and density. For example, in inflammatory dermatoses, the dermoscopic vascular structure may exhibit features such as dilatation and congestion, which are consistent with a histopathologic vascular inflammatory response.











